Fingertip digital thermal monitoring: a fingerprint for cardiovascular disease?
- Jan 10, 2023
- 3 min read
E E van der Wall, J D Schuijf, J J Bax, J W Jukema, M J Schalij
Int J Cardiovasc Imaging 2010 Feb;26(2):249-52.
Amongst the advanced cardiac imaging modalities, computed tomography (CT) angiography has emerged as a reliable non-invasive method for the assessment of coronary artery disease (CAD), coronary anatomy and cardiac function [1–17]. Multiple studies involving over several thousands of patients have established that CT angiography is highly accurate for delineation of the presence and severity of coronary atherosclerosis [18–23]. CT angiography may also reveal the total plaque burden, i.e. both calcified and non-calcified components, for individual patients with coronary atherosclerosis [24–35].
Coronary calcification is a marker of atherosclerosis that can be quantified with the use of cardiac CT and it is proportional to the extent and severity of atherosclerotic disease. Several large clinical trials found true incremental predictive value of coronary artery calcium over the Framingham risk score (FRS) when used in asymptomatic patients [36–40]. This relevant prognostic information may be used to initiate or intensify appropriate treatment strategies to slow the progression of atherosclerotic vascular disease. Current data suggests intermediate risk patients may benefit most from further risk stratification with cardiac CT, as coronary artery calcium testing is effective at identifying increased risk. Consequently, there is nowadays sufficient evidence that coronary artery calcium may be considered as useful predictor of coronary artery disease in certain at risk populations such as patients with diabetes, hypertension and in elderly patients [41–43].
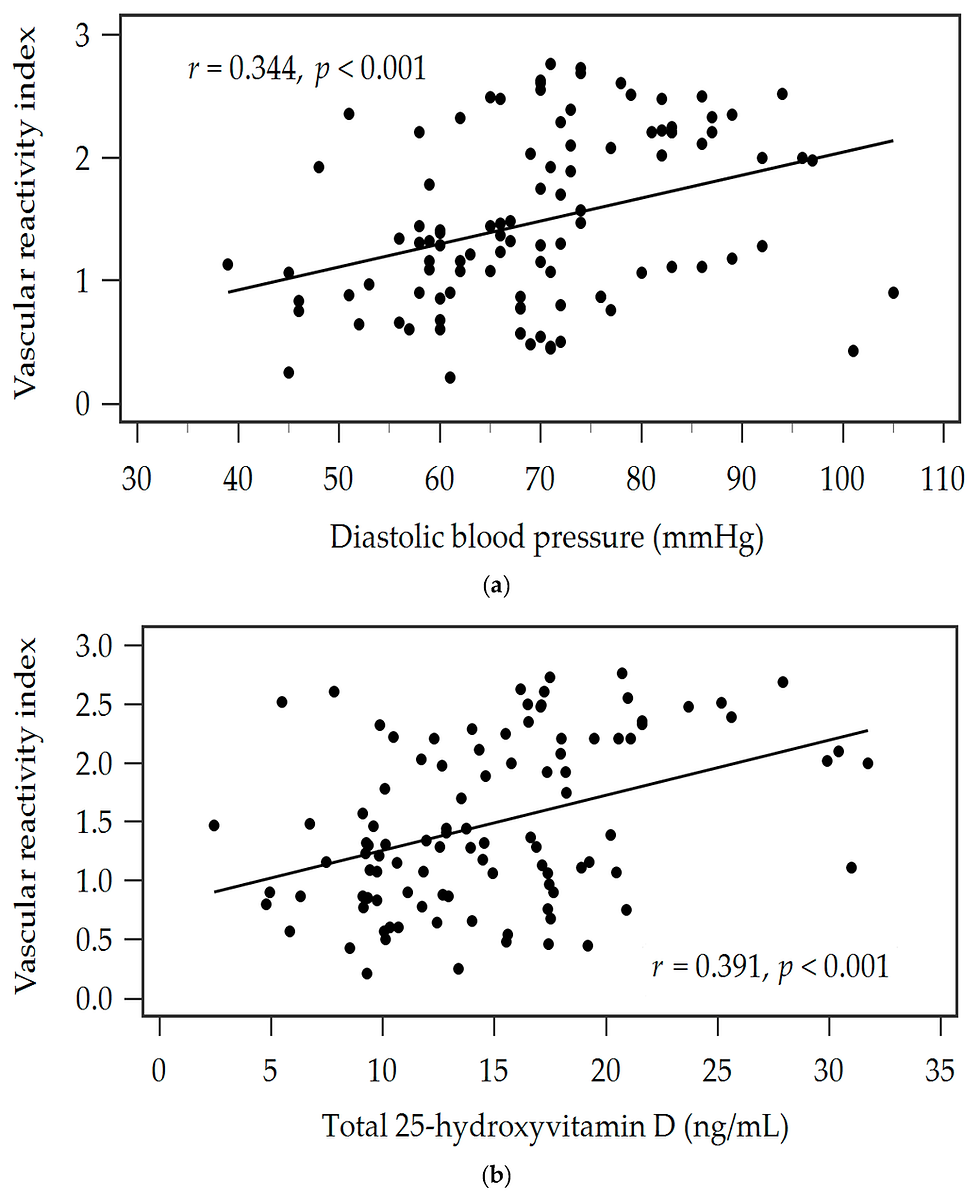
Vascular dysfunction is generally considered a key initial event in the atherosclerotic process which is a systemic disorder local manifestation. Functional changes in arteries precede the development of structural changes and also reverse more quickly in response to therapies [44]. Fingertip digital thermal monitoring (DTM) of vascular reactivity is a new non-invasive, operator-independent approach based on changes in fingertip temperature during and after arm cuff occlusion. DTM of vascular function during cuff-occlusive reactive hyperemia relies on the premise that changes in fingertip temperature during and after an ischemic stimulus reflect changes in blood flow. Vascular dysfunction measured by DTM has been shown to strongly correlate with FRS and coronary artery calcium independent of age, sex, and traditional cardiac risk factors and was superior to FRS for the prediction of significant coronary artery calcium [45].
In a previous issue of the International Journal of Cardiovascular Imaging Ahmadi et al. [46] evaluated the correlation between DTM and CAD measured by CT angiography in 129 symptomatic patients. The authors investigated the correlation between CT angiography and neurovascular reactivity measured by DTM. All DTM indices of vascular and neurovascular reactivity significantly decreased from normal to non-obstructive to obstructive CAD. Coronary artery calcium increased in each FRS category as vascular dysfunction increased. The most extensive CAD was observed in the group with maximum calcium score and vascular dysfunction, independent of age, gender and traditional cardiovascular risk factors. The authors concluded that vascular dysfunction measured by DTM provided incremental value over FRS for the detection of obstructive and non-obstructive CAD at CT angiography.
Previous studies from the same group had already shown strong correlations between low fingertip temperature rebound measured by DTM during a 5-minute arm-cuff induced reactive hyperemia and both the FRS, and coronary artery calcification in asymptomatic populations [47]. In another study, Amahdi et al. [48] did already demonstrate that vascular dysfunction measured by DTM was associated with the extent of myocardial perfusion defect independent of age, gender, and cardiac risk factors.
Although large prospective trials are needed to establish the true clinical value of fingertip DTM, the clinical implications are very promising. Patients at risk for CAD, such as patients with hypertension, metabolic syndrome and diabetes mellitus can be easily and noninvasively investigated with the patient-friendly fingertip DTM [49]. In these patients it is of paramount importance to measure and know the status of their vascular function. Fingertip DTM will also allow the evaluation of the effects of pharmacological drugs that influence vascular function. The current study by Ahmadi et al. [46] extends therefore previous findings that fingertip DTM is potentially valuable in the evaluation of at risk individuals in addition to risk factor measurement.
Read Full Text Here: https://link.springer.com/article/10.1007/s10554-009-9552-0


![Lipoprotein(a) levels predict endothelial dysfunction in maintenance hemodialysis patients: evidence from [VENDYS] vascular reactivity index assessment](https://static.wixstatic.com/media/dac531_5285607cc591409a9d83746f042af7c6~mv2.png/v1/fill/w_980,h_980,al_c,q_90,usm_0.66_1.00_0.01,enc_avif,quality_auto/dac531_5285607cc591409a9d83746f042af7c6~mv2.png)
Comments