Sensitivity of Digital Thermal Monitoring Parameters to Reactive Hyperemia
- Jan 10, 2023
- 2 min read
M. Akhtar, S. Kleis, R. Metcalfe, M. Naghavi
J Biomech Eng. May 2010, 132(5): 051005
Both structural and functional evaluations of the endothelium exist in order to diagnose cardiovascular disease (CVD) in its asymptomatic stages. Vascular reactivity, a functional evaluation of the endothelium in response to factors such as occlusion, cold, and stress, in addition to plasma markers, is the most widely accepted test and has been found to be a better predictor of the health of the endothelium than structural assessment tools such as coronary calcium scores or carotid intima-media thickness. Among the vascular reactivity assessment techniques available, digital thermal monitoring (DTM) is a noninvasive technique that measures the recovery of fingertip temperature after 2-5 min of brachial occlusion. On release of occlusion, the finger temperature responds to the amount of blood flow rate overshoot referred to as reactive hyperemia (RH), which has been shown to correlate with vascular health. Recent clinical trials have confirmed the potential importance of DTM as an early stage predictor of CVD. Numerical simulations of a finger were carried out to establish the relationship between DTM and RH. The model finger consisted of essential components including bone, tissue, major blood vessels (macrovasculature), skin, and microvasculature. The macrovasculature was represented by a pair of arteries and veins, while the microvasculature was represented by a porous medium. The time-dependent Navier-Stokes and energy equations were numerically solved to describe the temperature distribution in and around the finger. The blood flow waveform postocclusion, an input to the numerical model, was modeled as an instantaneous overshoot in flow rate (RH) followed by an exponential decay back to baseline flow rate. Simulation results were similar to clinically measured fingertip temperature profiles in terms of basic shape, temperature variations, and time delays at time scales associated with both heat conduction and blood perfusion. The DTM parameters currently in clinical use were evaluated and their sensitivity to RH was established. Among the parameters presented, temperature rebound (TR) was shown to have the best correlation with the level of RH with good sensitivity for the range of flow rates studied. It was shown that both TR and the equilibrium start temperature (representing the baseline flow rate) are necessary to identify the amount of RH and, thus, to establish criteria for predicting the state of specific patient's cardiovascular health.
Read Full Text Here: https://asmedigitalcollection.asme.org/biomechanical/article-abstract/132/5/051005/455708/Sensitivity-of-Digital-Thermal-Monitoring?redirectedFrom=fulltext


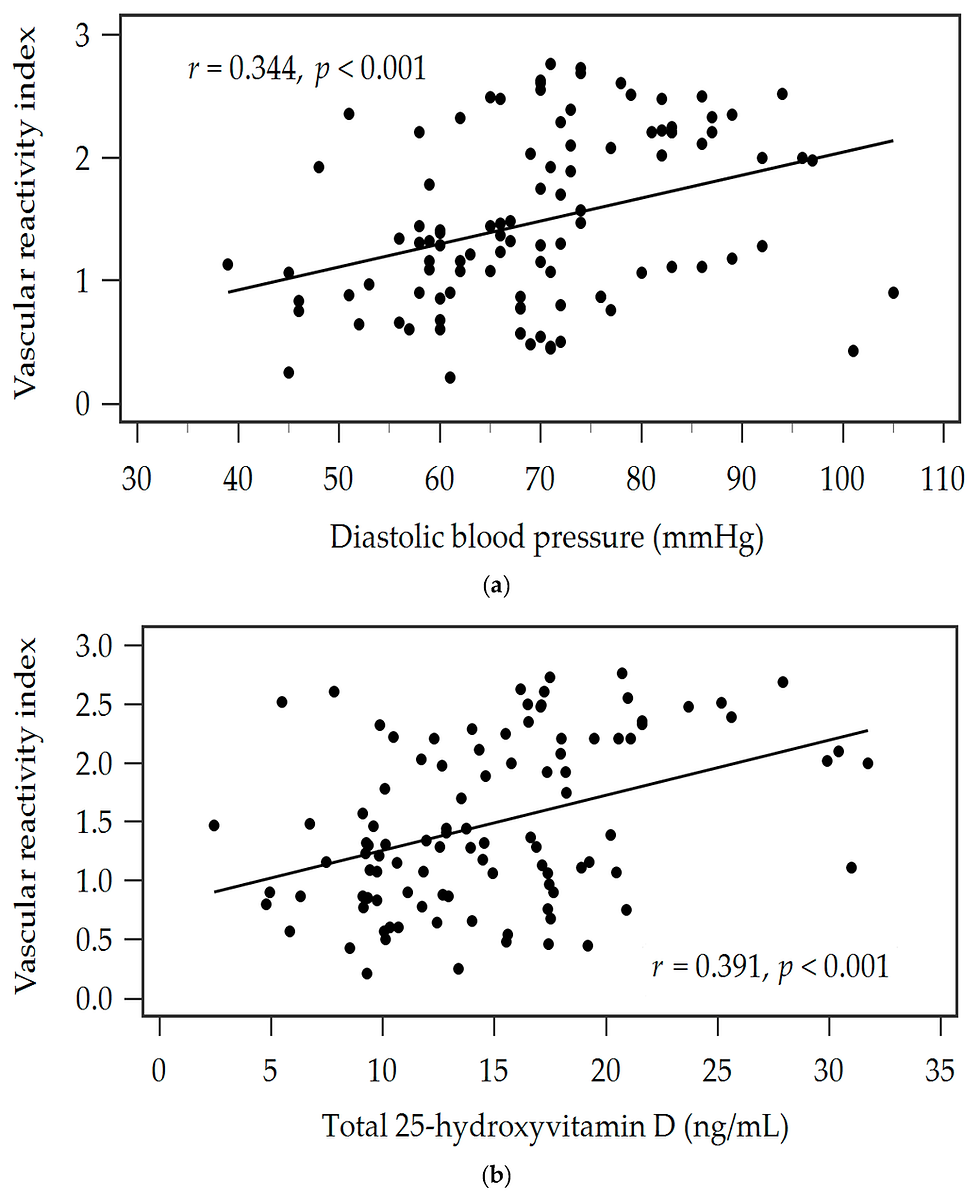
![Lipoprotein(a) levels predict endothelial dysfunction in maintenance hemodialysis patients: evidence from [VENDYS] vascular reactivity index assessment](https://static.wixstatic.com/media/dac531_5285607cc591409a9d83746f042af7c6~mv2.png/v1/fill/w_980,h_980,al_c,q_90,usm_0.66_1.00_0.01,enc_avif,quality_auto/dac531_5285607cc591409a9d83746f042af7c6~mv2.png)
Comments